Background: Cor-triatriatum is a rare congenital cardiac anomaly characterized by a fibromuscular membrane that divides the left atrium into two chambers, giving the appearance of three atrial compartments. It typically presents during infancy or childhood due to obstructive symptoms but may remain undiagnosed until adulthood in milder or non-obstructive cases. Case Presentation: A 33-year-old Ethiopian male with no known past medical history presented with a one-month history of progressive shortness of breath, orthopnea, paroxysmal nocturnal dyspnea, and bilateral leg swelling. He also reported a productive cough, pleuritic chest pain, and high-grade intermittent fever of similar duration. Physical examination and initial investigations suggested decompensated heart failure and pneumonia. Transthoracic echocardiography revealed findings consistent with cor-triatriatum sinister. Despite initiation of supportive care, intravenous antibiotics, diuretics, and mechanical ventilation, the patient’s condition deteriorated. He ultimately developed cardiogenic shock and died during hospitalization. Conclusion: Cor-triatriatum is a rare but important cause of heart failure in adult patients. This case demonstrates that congenital heart disease can remain clinically silent for decades and may present with acute decompensation. Awareness and early recognition of this anomaly, especially in resource-limited settings, are essential for timely diagnosis and management. Point-of-care ultrasound can be a valuable tool in such environments for rapid cardiac assessment and should be considered when evaluating patients with unexplained heart failure symptoms.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Atypical Cor Triatriatum Sinister, Heart Failure, Young Adult, Case Report
1. Introduction
Cor triatriatum is characterized by the existence of a fibromuscular membrane within either the left or right atrium, creating the appearance of three atria. It is associated with other cardiac anomalies in 80% of cases
[1]
P. N. Nassar, R. H. Hamdan, Cor Triatriatum Sinistrum: Classification and Imaging Modalities, Eur J Cardiovasc Med 1 (2011).
. The cause of cor triatriatum is not well understood, and several theories exist on the embryologic origin. The treatment for cor triatriatum may be aggressive or conservative and differs according to the severity of symptoms. Overall, in cases of isolated cor triatriatum, the prognosis is excellent. In most patients, the opening is severely restrictive and about 75% of those born with CT die in infancy. In rare cases, however, the onset of clinical manifestations may be delayed until adulthood if the opening is large. Such adults may be asymptomatic where the diagnosis is incidental,
[2]
S. R. Lindauer, Incidental finding of cor triatriatum sinistrum in an adult, Journal of Diagnostic Medical Sonography 30 (2014) 332-336.
the presenting clinical picture may be dyspnea, hemoptysis, heart failure,
[3]
E. Ilhan, M. Ergelen, Ö. Soylu, R. Tosu, T. S. Güvenç, Ş. Kul, T. Tezel, Severe right heart failure and pulmonary hypertension because of cor triatriatum sinister in a 54 year-old patient, Int J Cardiol 151 (2011).
pulmonary hypertension and/or atrial fibrillation. Here we report a case of 33 years old male patient who presented with heart failure in whom atypical cor triaatritum has been diagnosed due the vertical orientation of the dividing membrane, Illustrating very unusual and interesting case.
2. Case Presentation
A 33-year-old male patient presented to the emergency department with progressive fatigue, shortness of breath, orthopnea requiring two pillows, and paroxysmal nocturnal dyspnea (PND) that has persisted for one month. His symptoms have worsened over the past two weeks and are accompanied by swelling in both lower extremities. He also reports a productive cough that initially produced whitish, frothy sputum, which has since become blood-stained over the same time frame. Additionally, for the past week, he has experienced low-grade intermittent fever and sharp chest pain on both sides, which worsens with coughing.
For these compliant he sought treatment at a local general hospital, where he was admitted for two weeks and treated with antibiotics (ceftriaxone) and diuretics (furosemide). He was referred to our institution due to inadequate response to treatment. The patient has no prior history of similar complaints, chest heaviness, changes in eye color, hematemesis, diarrhea, constipation, changes in stool color, body weakness, abnormal movements, or urinary or stool incontinence. He also denies any history of dysuria, increased urinary frequency, or changes in urine color. There is no known history of chronic medical conditions in himself or his family. He works as a farmer in a rural area of Ethiopia and is the youngest child in his family. He is currently married but has no children.
Upon physical examination, the patient appeared acutely ill and was in respiratory distress, with a respiratory rate of 28 breaths per minute and an oxygen saturation of 94% while receiving 10 L of supplemental oxygen via a face mask. His blood pressure was 106/74 mmHg, pulse rate of 110 beats per minute, regular and full in volume, and a temperature of 36.9°C. Chest examination revealed absent air entry in the lower bilateral posterior two-thirds of the lungs, bronchial breath sounds were noted bilaterally over the upper third lung fields. The cardiovascular examination indicated raised jugular venous pressure at 5 cm above the sternal angle and a grade IV holosystolic murmur best heard at the apex, which radiated to the axilla. Abdominal examination showed a tender, palpable liver extending 5 cm below the right costal margin, with positive shifting dullness. The musculoskeletal examination revealed grade two bilateral pitting edema. No significant findings were noted in other systems.
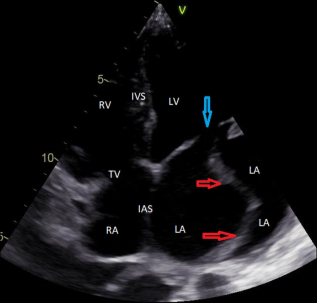
A bedside ultrasound (point-of-care ultrasound, POCUS) demonstrated bilateral pleural effusions with bilateral B-lines and signs of consolidative changes. The inferior vena cava appeared plethoric (diameter 2.53 cm) with minimal respiratory variation (10%), and there was visible membrane dividing the left atrium on the apical four-chamber view (Figure 1). Ejection fraction was estimated to be 35%. ECG showed a sinus tachycardia with rate of 112 bpm on monitor. High sensitive troponin was normal.
Figure 1. Transthoracic Echocardiography. Apical four chamber view demonstrating well-formed vertical membranous septum dividing the left atrium in to two (red arrow). Blue arrow, Mitral valve; RA, right atrium; LA, left atrium; LV, left ventricle; RV, right ventricle; IVS, inter-ventricular septum; IAS, inter-atrial septum.
The patient was diagnosed with NYHA class IV stage C heart failure secondary to congenital heart disease (CHD) due to cor triatriatum, along with hospital-acquired pneumonia (HAP). Diuretics (furosemide) were initiated at a dose of 80 mg Intravenous stat. The patient produced 250 ml of urine and was placed on furosemide 80 mg IV three times daily, along with spironolactone 25 mg orally once daily. Antibiotic therapy was adjusted to include ceftazidime 1 gm IV TID and vancomycin 1 gm IV BID, considering the diagnosis of hospital-acquired pneumonia after relevant investigations were sent (see Table 1).
The next day, despite the management provided, the patient's respiratory condition deteriorated, with the respiratory rate rising to 40. Blood pressure dropped to 85/60, and the patient became agitated, leading to the decision to intubate. After optimizing hemodynamic status, the patient was intubated and placed on mechanical ventilation. Norepinephrine was initiated at a dose of 0.05 mcg/kg/min, and due to the addition of a diagnosis of cardiogenic shock, the dosage was increased to achieve a mean arterial pressure (MAP) above 65. Unfortunately, the patient passed away despite efforts to optimize vasopressor support and antibiotic therapy.
Table 1. Investigation summary of the patient upon initial presentation.
Complete blood count
Patient value
WBC
10.3 × 103
Hemoglobin
12.7 g/dl
hematocrit
37.4%
Red blood cell
5.10 × 106
Platelet count
489 × 103
neutrophil
72.4%
lymphocyte
19.2%
eosinophil
2.8%
Creatinine
0.79 mg/dl
Urea
22.7 mg/dl
SGOT
17.4 IU/L
SGPT
7.5 IU/L
Total bilirubin
0.698 mg/dl
Albumin
2.65 g/dl
Serum electrolyte
sodium
131
potassium
2.86
chloride
86.2
Pleural fluid analysis
Cell count
900
Lymphocyte
80%
Neutrophil
20%
Protein
1.1 g/dl
Glucose
123 mg/dl
LDH
120 u/l
3. Discussion
Cor triatriatum is a rare cardiac anomaly that occurs when a fibromuscular membrane divides atrium into 2 distinct chambers
[1]
P. N. Nassar, R. H. Hamdan, Cor Triatriatum Sinistrum: Classification and Imaging Modalities, Eur J Cardiovasc Med 1 (2011).
. The membrane may be located in the right atrium (cor triatriatum dexter [CTD]) or left atrium (cor triatriatum sinister). CTS results from an improper merging of the common pulmonary vein with the left atrium during heart development, which is more commonly seen than CTD
[2]
S. R. Lindauer, Incidental finding of cor triatriatum sinistrum in an adult, Journal of Diagnostic Medical Sonography 30 (2014) 332-336.
. This cardiac anomaly was first described by Church in 1868 and reported to have an incidence of 0.4% at autopsy of patients with congenital cardiac disease and 0.2% among patients undergoing transesophageal echocardiography
[3]
E. Ilhan, M. Ergelen, Ö. Soylu, R. Tosu, T. S. Güvenç, Ş. Kul, T. Tezel, Severe right heart failure and pulmonary hypertension because of cor triatriatum sinister in a 54 year-old patient, Int J Cardiol 151 (2011).
. Although traditionally considered a pediatric condition, some cases remain undiagnosed until adulthood like in our patient due to mild or non-obstructive forms
[1]
P. N. Nassar, R. H. Hamdan, Cor Triatriatum Sinistrum: Classification and Imaging Modalities, Eur J Cardiovasc Med 1 (2011).
The severity of symptoms depends on the degree of obstruction caused by the membrane. Obstructive CTS presents with symptoms similar to mitral stenosis, including progressive dyspnea, orthopnea, PND, and exercise intolerance,
[3]
E. Ilhan, M. Ergelen, Ö. Soylu, R. Tosu, T. S. Güvenç, Ş. Kul, T. Tezel, Severe right heart failure and pulmonary hypertension because of cor triatriatum sinister in a 54 year-old patient, Int J Cardiol 151 (2011).
. Non-obstructive CTS can remain asymptomatic and be detected incidentally during echocardiography
[8]
N. Alphonso, M. A. Nørgaard, A. Newcomb, Y. D’Udekem, C. P. Brizard, A. Cochrane, Cor triatriatum: Presentation, diagnosis and long-term surgical results, Annals of Thoracic Surgery 80 (2005) 1666-1671.
. Cases of atrial fibrillation, systemic embolism, and infective endocarditis due to stasis in the accessory left atrial chamber have also been reported
[9]
N. Nawaz, A. Jones, ATRIAL FIBRILLATION COMPLEX CASE STUDY Cor Triatriatum Sinister in an 88-year-old Male with New-onset Atrial Fibrillation, (n. d.).
R. Hamdan, N. Mirochnik, D. Celermajer, P. Nassar, L. Iserin, Cor Triatriatum Sinister diagnosed in adult life with three dimensional transesophageal echocardiography., BMC Cardiovasc Disord 10 (2010) 54.
. This aligns with our patient’s presentation and highlights the rarity of the case as he remained undiagnosed until adulthood.
The diagnosis is usually established by 2 D TTE (2-dimensional transthoracic echocardiography). Color flow mapping usually demonstrates increases in velocity and turbulent flow, suggesting obstruction that can be assessed by continuous wave Doppler through the membrane
[11]
M. S. Tsai, W. J. Chen, C. H. Huang, Cor Triatriatum in an adult with late presentation of symptoms, J Med Ultrasound 21 (2013) 156-158.
. Transesophageal echocardiography is superior to transthoracic imaging to diagnose cor triatriatum, providing better imaging of the left atria, left atria appendage, morphology of the dividing membrane and the degree of obstruction.
[12]
J. Kokotsakis, V. Anagnostakou, G. Almpanis, I. Paralikas, I. Nenekidis, T. Kratimenos, E. Prapa, N. Tragotsalou, A. Lioulias, A. Mazarakis, Cor triatriatum presenting as heart failure with reduced ejection fraction: A case report, J Cardiothorac Surg 6 (2011).
. Three D echocardiography is a more recent diagnostic tool providing additional information, able to demonstrate the entire membrane, the size, the location and the number of openings in the dividing membrane
[12]
J. Kokotsakis, V. Anagnostakou, G. Almpanis, I. Paralikas, I. Nenekidis, T. Kratimenos, E. Prapa, N. Tragotsalou, A. Lioulias, A. Mazarakis, Cor triatriatum presenting as heart failure with reduced ejection fraction: A case report, J Cardiothorac Surg 6 (2011).
. It also provides superior anatomical detail, distinguishing CTS from other conditions such as mitral stenosis or supravalvular mitral rings
[8]
N. Alphonso, M. A. Nørgaard, A. Newcomb, Y. D’Udekem, C. P. Brizard, A. Cochrane, Cor triatriatum: Presentation, diagnosis and long-term surgical results, Annals of Thoracic Surgery 80 (2005) 1666-1671.
A. Thakrar, M. D. Shapiro, D. S. Jassal, T. G. Neilan, M. Etta, E. King, S. Abbara, Cor triatriatum: The utility of cardiovascular imaging, 2007.
[5, 13]
. Histopathological examination post-surgery reveals a fibromuscular membrane composed of endocardial tissue without valvular structures, confirming the diagnosis
[14]
E. Einav, G. Perk, I. Kronzon, Three-dimensional transthoracic echocardiographic evaluation of cor triatriatum, European Journal of Echocardiography 9 (2008) 110-112.
. In our patient, further investigations were not possible due to the patient’s critical condition, making transport unsafe. However, bedside echocardiography revealed a well-formed, vertically oriented membrane in the left atrium (Figure 1). Additionally, cardiac MRI and histopathology could not be conducted because these resources were unavailable.
The primary treatment for symptomatic CTS is surgical resection of the membrane, which provides definitive relief
[1]
P. N. Nassar, R. H. Hamdan, Cor Triatriatum Sinistrum: Classification and Imaging Modalities, Eur J Cardiovasc Med 1 (2011).
. Medical management (diuretics, anticoagulation, and heart failure therapy) may be used for symptomatic relief but does not address the underlying defect
[7]
O. Işik, M. Akyüz, M. F. Ayik, E. Levent, Y. Atay, Cor triatriatum sinister: A case series, Turk Kardiyoloji Dernegi Arsivi 44 (2016) 20-23.
. In cases of concomitant cardiac surgery (e.g., mitral valve repair or atrial fibrillation ablation), CTS correction is often performed simultaneously
[13]
A. Thakrar, M. D. Shapiro, D. S. Jassal, T. G. Neilan, M. Etta, E. King, S. Abbara, Cor triatriatum: The utility of cardiovascular imaging, 2007.
[13]
. There are also rare reports of successful balloon catheter dilation of the communication between the proximal and distal chambers, but the long-term outcomes are yet to be determined
[15]
L. Di Bacco, M. D’Alonzo, A. Repossini, F. Zanin, C. Muneretto, S. Benussi, Treatment of non-restrictive cor triatriatum sinister during concomitant cardiac surgery, The Cardiothoracic Surgeon 30 (2022).
. In our case, the patient presented with congestion and was treated medically with diuretics and antibiotics due to an additional diagnosis of a hospital-acquired infection.
Reported long-term results of surgery are excellent low rates of perioperative mortality and considerable symptomatic relief
[5]
S A DOXIADIS, & J L EMERY. (1953). A case of triatrial heart. The Journal of Pediatrics, 42(1), 87-91.
. Long-term survival following membrane resection is similar to that of the general population, as long as there is no remaining obstruction or pulmonary hypertension
[10]
R. Hamdan, N. Mirochnik, D. Celermajer, P. Nassar, L. Iserin, Cor Triatriatum Sinister diagnosed in adult life with three dimensional transesophageal echocardiography., BMC Cardiovasc Disord 10 (2010) 54.
. Patients who are diagnosed and treated prior to the development of severe pulmonary hypertension tend to have the most favorable prognosis
[10]
R. Hamdan, N. Mirochnik, D. Celermajer, P. Nassar, L. Iserin, Cor Triatriatum Sinister diagnosed in adult life with three dimensional transesophageal echocardiography., BMC Cardiovasc Disord 10 (2010) 54.
This case report has limitations arising from the lack of additional investigations that could have provided a more detailed characterization of the cardiac lesion, such as cardiac MRI and post-mortem histological examination of the tissue. Furthermore, the patient's critical condition and the unavailability of such investigations rendered surgical management unfeasible.
4. Conclusion
Cor triatriatum is a rare cardiac anomaly characterized by a fibromuscular membrane that divides the atrium into two chambers. Although typically diagnosed in children, some cases, like that of our patient, remain undetected until adulthood. The severity of symptoms correlates with the degree of obstruction caused by the membrane. Diagnosis is usually confirmed through 2D transthoracic echocardiography, while histopathological examination post-surgery reveals a fibromuscular membrane made of endocardial tissue without valvular structures. In resource-limited settings like ours, bedside echocardiography and clinical findings play a crucial role. Surgical resection of the membrane is the primary treatment for symptomatic cases and provides definitive relief, while medical management are for symptom control. Long-term outcomes following surgery are generally excellent.
Abbreviations
PND
Paroxysmal Nocturnal Dyspnea
NYHA
New York Heart Association
HAP
Hospital Acquired Pneumonia
CHD
Congenital Heart Disease
ECG
Electrocardiography
MAP
Mean Arterial Pressure
CTD
Cor Triatriatum Dexter
CTS
Cor Triatriatum Sinister
2DTTE
2 Dimensional Transthoracic Echocardiography
MRI
Magnetic Resonance Imaging
Author Contributions
Amanuel Dagabas Wakoya: Conceptualization, Data curation, Writing – original draft
Ayto Addisu Negash: Conceptualization, Data curation
E. Ilhan, M. Ergelen, Ö. Soylu, R. Tosu, T. S. Güvenç, Ş. Kul, T. Tezel, Severe right heart failure and pulmonary hypertension because of cor triatriatum sinister in a 54 year-old patient, Int J Cardiol 151 (2011).
N. Alphonso, M. A. Nørgaard, A. Newcomb, Y. D’Udekem, C. P. Brizard, A. Cochrane, Cor triatriatum: Presentation, diagnosis and long-term surgical results, Annals of Thoracic Surgery 80 (2005) 1666-1671.
N. Nawaz, A. Jones, ATRIAL FIBRILLATION COMPLEX CASE STUDY Cor Triatriatum Sinister in an 88-year-old Male with New-onset Atrial Fibrillation, (n. d.).
R. Hamdan, N. Mirochnik, D. Celermajer, P. Nassar, L. Iserin, Cor Triatriatum Sinister diagnosed in adult life with three dimensional transesophageal echocardiography., BMC Cardiovasc Disord 10 (2010) 54.
J. Kokotsakis, V. Anagnostakou, G. Almpanis, I. Paralikas, I. Nenekidis, T. Kratimenos, E. Prapa, N. Tragotsalou, A. Lioulias, A. Mazarakis, Cor triatriatum presenting as heart failure with reduced ejection fraction: A case report, J Cardiothorac Surg 6 (2011).
A. Thakrar, M. D. Shapiro, D. S. Jassal, T. G. Neilan, M. Etta, E. King, S. Abbara, Cor triatriatum: The utility of cardiovascular imaging, 2007.
[14]
E. Einav, G. Perk, I. Kronzon, Three-dimensional transthoracic echocardiographic evaluation of cor triatriatum, European Journal of Echocardiography 9 (2008) 110-112.
L. Di Bacco, M. D’Alonzo, A. Repossini, F. Zanin, C. Muneretto, S. Benussi, Treatment of non-restrictive cor triatriatum sinister during concomitant cardiac surgery, The Cardiothoracic Surgeon 30 (2022).
Wakoya, A. D., Negash, A. A., Abebe, Z. A., Assefa, F. N., Getahun, Z., et al. (2025). A Case of Atypical Cor Triatriatum Sinister Persisting into Adulthood. International Journal of Clinical and Experimental Medical Sciences, 11(2), 23-27. https://doi.org/10.11648/j.ijcems.20251102.12
Wakoya, A. D.; Negash, A. A.; Abebe, Z. A.; Assefa, F. N.; Getahun, Z., et al. A Case of Atypical Cor Triatriatum Sinister Persisting into Adulthood. Int. J. Clin. Exp. Med. Sci.2025, 11(2), 23-27. doi: 10.11648/j.ijcems.20251102.12
Wakoya AD, Negash AA, Abebe ZA, Assefa FN, Getahun Z, et al. A Case of Atypical Cor Triatriatum Sinister Persisting into Adulthood. Int J Clin Exp Med Sci. 2025;11(2):23-27. doi: 10.11648/j.ijcems.20251102.12
@article{10.11648/j.ijcems.20251102.12,
author = {Amanuel Dagabas Wakoya and Ayto Addisu Negash and Zebideru Alayuu Abebe and Fitsum Negusse Assefa and Zelalem Getahun and Alemu Bimrew Mesekere},
title = {A Case of Atypical Cor Triatriatum Sinister Persisting into Adulthood
},
journal = {International Journal of Clinical and Experimental Medical Sciences},
volume = {11},
number = {2},
pages = {23-27},
doi = {10.11648/j.ijcems.20251102.12},
url = {https://doi.org/10.11648/j.ijcems.20251102.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcems.20251102.12},
abstract = {Background: Cor-triatriatum is a rare congenital cardiac anomaly characterized by a fibromuscular membrane that divides the left atrium into two chambers, giving the appearance of three atrial compartments. It typically presents during infancy or childhood due to obstructive symptoms but may remain undiagnosed until adulthood in milder or non-obstructive cases. Case Presentation: A 33-year-old Ethiopian male with no known past medical history presented with a one-month history of progressive shortness of breath, orthopnea, paroxysmal nocturnal dyspnea, and bilateral leg swelling. He also reported a productive cough, pleuritic chest pain, and high-grade intermittent fever of similar duration. Physical examination and initial investigations suggested decompensated heart failure and pneumonia. Transthoracic echocardiography revealed findings consistent with cor-triatriatum sinister. Despite initiation of supportive care, intravenous antibiotics, diuretics, and mechanical ventilation, the patient’s condition deteriorated. He ultimately developed cardiogenic shock and died during hospitalization. Conclusion: Cor-triatriatum is a rare but important cause of heart failure in adult patients. This case demonstrates that congenital heart disease can remain clinically silent for decades and may present with acute decompensation. Awareness and early recognition of this anomaly, especially in resource-limited settings, are essential for timely diagnosis and management. Point-of-care ultrasound can be a valuable tool in such environments for rapid cardiac assessment and should be considered when evaluating patients with unexplained heart failure symptoms.},
year = {2025}
}
TY - JOUR
T1 - A Case of Atypical Cor Triatriatum Sinister Persisting into Adulthood
AU - Amanuel Dagabas Wakoya
AU - Ayto Addisu Negash
AU - Zebideru Alayuu Abebe
AU - Fitsum Negusse Assefa
AU - Zelalem Getahun
AU - Alemu Bimrew Mesekere
Y1 - 2025/08/11
PY - 2025
N1 - https://doi.org/10.11648/j.ijcems.20251102.12
DO - 10.11648/j.ijcems.20251102.12
T2 - International Journal of Clinical and Experimental Medical Sciences
JF - International Journal of Clinical and Experimental Medical Sciences
JO - International Journal of Clinical and Experimental Medical Sciences
SP - 23
EP - 27
PB - Science Publishing Group
SN - 2469-8032
UR - https://doi.org/10.11648/j.ijcems.20251102.12
AB - Background: Cor-triatriatum is a rare congenital cardiac anomaly characterized by a fibromuscular membrane that divides the left atrium into two chambers, giving the appearance of three atrial compartments. It typically presents during infancy or childhood due to obstructive symptoms but may remain undiagnosed until adulthood in milder or non-obstructive cases. Case Presentation: A 33-year-old Ethiopian male with no known past medical history presented with a one-month history of progressive shortness of breath, orthopnea, paroxysmal nocturnal dyspnea, and bilateral leg swelling. He also reported a productive cough, pleuritic chest pain, and high-grade intermittent fever of similar duration. Physical examination and initial investigations suggested decompensated heart failure and pneumonia. Transthoracic echocardiography revealed findings consistent with cor-triatriatum sinister. Despite initiation of supportive care, intravenous antibiotics, diuretics, and mechanical ventilation, the patient’s condition deteriorated. He ultimately developed cardiogenic shock and died during hospitalization. Conclusion: Cor-triatriatum is a rare but important cause of heart failure in adult patients. This case demonstrates that congenital heart disease can remain clinically silent for decades and may present with acute decompensation. Awareness and early recognition of this anomaly, especially in resource-limited settings, are essential for timely diagnosis and management. Point-of-care ultrasound can be a valuable tool in such environments for rapid cardiac assessment and should be considered when evaluating patients with unexplained heart failure symptoms.
VL - 11
IS - 2
ER -
Wakoya, A. D., Negash, A. A., Abebe, Z. A., Assefa, F. N., Getahun, Z., et al. (2025). A Case of Atypical Cor Triatriatum Sinister Persisting into Adulthood. International Journal of Clinical and Experimental Medical Sciences, 11(2), 23-27. https://doi.org/10.11648/j.ijcems.20251102.12
Wakoya, A. D.; Negash, A. A.; Abebe, Z. A.; Assefa, F. N.; Getahun, Z., et al. A Case of Atypical Cor Triatriatum Sinister Persisting into Adulthood. Int. J. Clin. Exp. Med. Sci.2025, 11(2), 23-27. doi: 10.11648/j.ijcems.20251102.12
Wakoya AD, Negash AA, Abebe ZA, Assefa FN, Getahun Z, et al. A Case of Atypical Cor Triatriatum Sinister Persisting into Adulthood. Int J Clin Exp Med Sci. 2025;11(2):23-27. doi: 10.11648/j.ijcems.20251102.12
@article{10.11648/j.ijcems.20251102.12,
author = {Amanuel Dagabas Wakoya and Ayto Addisu Negash and Zebideru Alayuu Abebe and Fitsum Negusse Assefa and Zelalem Getahun and Alemu Bimrew Mesekere},
title = {A Case of Atypical Cor Triatriatum Sinister Persisting into Adulthood
},
journal = {International Journal of Clinical and Experimental Medical Sciences},
volume = {11},
number = {2},
pages = {23-27},
doi = {10.11648/j.ijcems.20251102.12},
url = {https://doi.org/10.11648/j.ijcems.20251102.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcems.20251102.12},
abstract = {Background: Cor-triatriatum is a rare congenital cardiac anomaly characterized by a fibromuscular membrane that divides the left atrium into two chambers, giving the appearance of three atrial compartments. It typically presents during infancy or childhood due to obstructive symptoms but may remain undiagnosed until adulthood in milder or non-obstructive cases. Case Presentation: A 33-year-old Ethiopian male with no known past medical history presented with a one-month history of progressive shortness of breath, orthopnea, paroxysmal nocturnal dyspnea, and bilateral leg swelling. He also reported a productive cough, pleuritic chest pain, and high-grade intermittent fever of similar duration. Physical examination and initial investigations suggested decompensated heart failure and pneumonia. Transthoracic echocardiography revealed findings consistent with cor-triatriatum sinister. Despite initiation of supportive care, intravenous antibiotics, diuretics, and mechanical ventilation, the patient’s condition deteriorated. He ultimately developed cardiogenic shock and died during hospitalization. Conclusion: Cor-triatriatum is a rare but important cause of heart failure in adult patients. This case demonstrates that congenital heart disease can remain clinically silent for decades and may present with acute decompensation. Awareness and early recognition of this anomaly, especially in resource-limited settings, are essential for timely diagnosis and management. Point-of-care ultrasound can be a valuable tool in such environments for rapid cardiac assessment and should be considered when evaluating patients with unexplained heart failure symptoms.},
year = {2025}
}
TY - JOUR
T1 - A Case of Atypical Cor Triatriatum Sinister Persisting into Adulthood
AU - Amanuel Dagabas Wakoya
AU - Ayto Addisu Negash
AU - Zebideru Alayuu Abebe
AU - Fitsum Negusse Assefa
AU - Zelalem Getahun
AU - Alemu Bimrew Mesekere
Y1 - 2025/08/11
PY - 2025
N1 - https://doi.org/10.11648/j.ijcems.20251102.12
DO - 10.11648/j.ijcems.20251102.12
T2 - International Journal of Clinical and Experimental Medical Sciences
JF - International Journal of Clinical and Experimental Medical Sciences
JO - International Journal of Clinical and Experimental Medical Sciences
SP - 23
EP - 27
PB - Science Publishing Group
SN - 2469-8032
UR - https://doi.org/10.11648/j.ijcems.20251102.12
AB - Background: Cor-triatriatum is a rare congenital cardiac anomaly characterized by a fibromuscular membrane that divides the left atrium into two chambers, giving the appearance of three atrial compartments. It typically presents during infancy or childhood due to obstructive symptoms but may remain undiagnosed until adulthood in milder or non-obstructive cases. Case Presentation: A 33-year-old Ethiopian male with no known past medical history presented with a one-month history of progressive shortness of breath, orthopnea, paroxysmal nocturnal dyspnea, and bilateral leg swelling. He also reported a productive cough, pleuritic chest pain, and high-grade intermittent fever of similar duration. Physical examination and initial investigations suggested decompensated heart failure and pneumonia. Transthoracic echocardiography revealed findings consistent with cor-triatriatum sinister. Despite initiation of supportive care, intravenous antibiotics, diuretics, and mechanical ventilation, the patient’s condition deteriorated. He ultimately developed cardiogenic shock and died during hospitalization. Conclusion: Cor-triatriatum is a rare but important cause of heart failure in adult patients. This case demonstrates that congenital heart disease can remain clinically silent for decades and may present with acute decompensation. Awareness and early recognition of this anomaly, especially in resource-limited settings, are essential for timely diagnosis and management. Point-of-care ultrasound can be a valuable tool in such environments for rapid cardiac assessment and should be considered when evaluating patients with unexplained heart failure symptoms.
VL - 11
IS - 2
ER -