1. Introduction
Conjunctivitis is characterized by the inflammation of the conjunctiva, the lining of the eyelids and eyeball, caused by bacteria or viruses, allergic and immunological reactions, among other potential factors
| [1] | Sambursky, R. Acute Conjunctivitis. BMJ Best Practice. 2019, 1–55. |
| [2] | Jacobs, D. S. Conjunctivitis. 2020, 1–24. |
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
[1-3]
. The disorder can be classified and identified based on the agent causing the inflammation and the symptoms presented
| [1] | Sambursky, R. Acute Conjunctivitis. BMJ Best Practice. 2019, 1–55. |
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [4] | Bielory, L., Delgado, L., Katelaris, C. H., Leonardi, A., Rosario, N., & Vichyanoud, P. ICON: Diagnosis and Management of Allergic Conjunctivitis. Ann Allergy Asthma Immunol. 2020, 124(2), 118–134.
https://doi.org/10.1016/j.anai.2019.11.014 |
[1, 3, 4]
.
This disorder affects a large part of the population, mainly in its acute allergic, infectious bacterial and viral forms, representing 54% of visits to basic health units related to eye conditions and 30% of visits to the emergency room
| [1] | Sambursky, R. Acute Conjunctivitis. BMJ Best Practice. 2019, 1–55. |
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [4] | Bielory, L., Delgado, L., Katelaris, C. H., Leonardi, A., Rosario, N., & Vichyanoud, P. ICON: Diagnosis and Management of Allergic Conjunctivitis. Ann Allergy Asthma Immunol. 2020, 124(2), 118–134.
https://doi.org/10.1016/j.anai.2019.11.014 |
[1, 3, 4]
. In the United States, it is estimated that acute conjunctivitis affects around six million people per year
.
Despite being a self-limiting disease, it can cause significant suffering in individuals who develop it. Furthermore, there is the possibility of a variable economic loss, considering the symptoms presented and their duration
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [6] | Hamrah, P. & Dana, R. Allergic Conjunctivitis: Clinical Manifestations and Diagnosis. 2020, p. 13. Available from: https://medilib.ir/uptodate/show/5547 (Accessed 2020 Jan 06). |
[3, 6]
. The costs involved can be direct, such as medical appointments and medications, or indirect, such as days lost at work and at school, in addition to reduced productivity during work
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [6] | Hamrah, P. & Dana, R. Allergic Conjunctivitis: Clinical Manifestations and Diagnosis. 2020, p. 13. Available from: https://medilib.ir/uptodate/show/5547 (Accessed 2020 Jan 06). |
[3, 6]
.
Therefore, appropriate symptomatic management of this disease is necessary. To guide this clinical management and standardize the best care provided to the patient, health professionals can resort to the implementation of protocols and/or clinical practice guidelines based on quality scientific evidence, to optimize patient care, translating practice of Evidence-Based Health (EBH)
| [7] | Galvão, M., Sawada, O. & Rossí, A. Evidence-Based Practice: Theoretical Considerations for Its Implementation in Perioperative Nursing. Rev Lat Am Enfermagem. 2002, 10, 690–695. https://doi.org/10.1590/S0104-11692002000500010 |
| [8] | Migowski, A. Methodological Guidelines: Preparation of Clinical Guidelines. Rev Bras Cancerol. 2016, 62, 165–166. |
| [9] | Shaneyfelt, T., Smith, M. & Rothwangl, J. Are Guidelines Following Guidelines? The Methodological Quality of Clinical Practice Guidelines in the Peer-Reviewed Medical Literature. 1999, 281–20. |
| [10] | Djulbegovic, B. & Guyatt, G. H. Progress in Evidence-Based Medicine: A Quarter Century On. Lancet. 2017, 390(10092), 415–423. https://doi.org/10.1016/S0140-6736(16)31592-6 |
| [11] | Hoffmann-Eßer, W., Siering, U., Neugebauer, E. A., Brockhaus, A. C., Lampert, U. & Eikermann, M. Guideline Appraisal with AGREE II: Systematic Review of the Current Evidence on How Users Handle the 2 Overall Assessments. PLoS ONE. 2017, 12(3), e0174831.
https://doi.org/10.1371/journal.pone.0174831 |
[7-11]
.
EBH, therefore, is the result of a movement that seeks to guide health professionals about the best clinical decision, according to the patient's specific condition
| [2] | Jacobs, D. S. Conjunctivitis. 2020, 1–24. |
[2]
. It has a solid scientific basis and the development of more sophisticated hierarchies of evidence, which respects the patient's values and preferences when making decisions, capable of generating reliable and safe recommendations
| [7] | Galvão, M., Sawada, O. & Rossí, A. Evidence-Based Practice: Theoretical Considerations for Its Implementation in Perioperative Nursing. Rev Lat Am Enfermagem. 2002, 10, 690–695. https://doi.org/10.1590/S0104-11692002000500010 |
| [10] | Djulbegovic, B. & Guyatt, G. H. Progress in Evidence-Based Medicine: A Quarter Century On. Lancet. 2017, 390(10092), 415–423. https://doi.org/10.1016/S0140-6736(16)31592-6 |
[7, 10]
. Its application in the health professional's routine is through clinical practice guidelines or protocols, which play great importance in the management and prevention of a considerable variety of diseases
| [10] | Djulbegovic, B. & Guyatt, G. H. Progress in Evidence-Based Medicine: A Quarter Century On. Lancet. 2017, 390(10092), 415–423. https://doi.org/10.1016/S0140-6736(16)31592-6 |
| [13] | Duarte, G. S., Delgado, R. M., Costa, J. & Vaz-Carneiro, A. Analysis of the Cochrane Review: Non-Medical Prescribing versus Medical Prescribing for the Management of Acute and Chronic Diseases in Primary and Secondary Health Care. Cochrane Database Syst Rev. 2017, 7–11. |
| [14] | Santana, R. S., de Oliveira Lupatini, E., Zanghelini, F., de March Ronsoni, R., Rech, N. & Leite, S. N. The Different Clinical Guideline Standards in Brazil: High Cost Treatment Diseases versus Poverty-Related Diseases. PLoS One. 2028, 13(10), e0204723.
https://doi.org/10.1371/journal.pone.0204723 |
| [15] | AGREE Next Steps Consortium. The AGREE II Instrument. 2009. Available from: http://www.agreetrust.org (Accessed 2020 Aug 24). |
[10, 13-15]
.
However, a factor that hinders the effective application of the guidelines is the varying quality of the recommendations presented
| [13] | Duarte, G. S., Delgado, R. M., Costa, J. & Vaz-Carneiro, A. Analysis of the Cochrane Review: Non-Medical Prescribing versus Medical Prescribing for the Management of Acute and Chronic Diseases in Primary and Secondary Health Care. Cochrane Database Syst Rev. 2017, 7–11. |
| [15] | AGREE Next Steps Consortium. The AGREE II Instrument. 2009. Available from: http://www.agreetrust.org (Accessed 2020 Aug 24). |
[13, 15]
. Several guidelines developed for the care of the same disease can be produced with different methods and objectives, generating competition and a complex system of conflicting practices and interventions, in addition to a lack of methodological rigor and transparency in their preparation
| [15] | AGREE Next Steps Consortium. The AGREE II Instrument. 2009. Available from: http://www.agreetrust.org (Accessed 2020 Aug 24). |
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
[15, 16]
. The main attributes of high-quality guidelines include validation, reliability, reproducibility, clinical applicability, adaptation to the health context, clarity, multidisciplinary character, evidence review and documentation
| [17] | Vaz, J. M., Alves, B. M., Duarte, D. B., Marques, L. A. & Santana, R. S. Quality Appraisal of Existing Guidelines for the Management of Headache Disorders by the AGREE II’s Method. Cephalalgia. 2022, 42(3), 239–249.
https://doi.org/10.1177/03331024211056694 |
| [18] | Alnamankany, A. & Ashley, P. Assessment of the Quality of Reporting of Randomized Clinical Trials in Paediatric Dentistry: A Comparative Systematic Review. Taibah Univ Med Sci. 2020, 15(1), 1–7.
https://doi.org/10.1016/j.jtumed.2019.12.001 |
[17, 18]
.
In the era of EBH and with the increase in the number of publications, the critical evaluation of evidence must be considered before its application, especially regarding health care, referring to self-limited diseases
| [12] | Zeng, X., Zhang, Y., Kwong, J. S., Zhang, C., Li, S., Sun, F., et al. The Methodological Quality Assessment Tools for Preclinical and Clinical Studies, Systematic Review and Meta-Analysis, and Clinical Practice Guideline: A Systematic Review. J Evid Based Med. 2015, 8(1), 2–10.
https://doi.org/10.1111/jebm.12141 |
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
| [19] | Anwer, M. A., Al-Fahed, O. B., Arif, S. I., Amer, Y. S., Titi, M. A. & Al-Rukban, M. O. Quality Assessment of Recent Evidence-Based Clinical Practice Guidelines for Management of Type 2 Diabetes Mellitus in Adults Using the AGREE II Instrument. J Eval Clin Pract. 2018, 24(1), 166–172.
https://doi.org/10.1111/jep.12832 |
[12, 16, 19]
. In this context, the objective of this study was to systematically identify guidelines and/or clinical protocols on the management of primary conjunctivitis and critically evaluate their quality.
2. Methods
2.1. Identification and Selection of Clinical Guidelines
A systematic search was carried out in the literature between the months of January and August 2020 using the Decs/Mesh descriptors related to the topic: "Conjunctivitis" OR "Conjunctivitides" OR “Conjuntivite”. To search for clinical practice guidelines (CPG) for the management of conjunctivitis in the following databases: Medscape (filter: Diseases/Conditions, past year), Best Medicine Journal (BMJ), UpToDate, PubMed (filter: 10 years, Practice Guideline, Pragmatic Clinical Trial) and Biblioteca Virtual em Saúde (BVS).
In addition, searches were carried out on specific websites of health institutions and categories: Cochrane (filter: Protocol), Comissão Nacional de Incorporação de Tecnologias (CONITEC) in Sistema Único de Saúde (SUS) (filter: Guideline) and National Institute for Health and Clinical Excellence (NICE). In a second step, another evaluation of texts found in the PubMed database was carried out, according to the reference suggestions from one of the selected texts, “Guidelines for the clinical management of allergic conjunctival disease” (2nd edition).
The articles were filtered based on language (Portuguese and English) and publication time (last 10 years). Guidelines and review articles containing recommendations, pharmacological or non-pharmacological, related to the management of acute conjunctivitis in adults, whose presentations can be allergic, bacterial or viral, were included. As exclusion criteria, we used: publications whose scope did not encompass the acute treatment of conjunctivitis, documents aimed at specific populations, such as children and pregnant women, in addition to articles unavailable in full. The selection was carried out by two researchers independently, using the Rayyan web application, where duplication was excluded, followed by reading and analyzing titles and abstracts using the application. After selecting the guidelines, the selected documents were fully read and analyzed.
2.2. Appraisal of Guidelines for Research & Evaluation (AGREE II)
The AGREE II (Appraisal of Guidelines for Research & Evaluation) instrument aims to evaluate methodological quality and transparency in the development of clinical guidelines
| [8] | Migowski, A. Methodological Guidelines: Preparation of Clinical Guidelines. Rev Bras Cancerol. 2016, 62, 165–166. |
| [15] | AGREE Next Steps Consortium. The AGREE II Instrument. 2009. Available from: http://www.agreetrust.org (Accessed 2020 Aug 24). |
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
[8, 15, 16]
. This can be applied to guidelines related to any disease and any stage of health care, including aspects related to health promotion, public health, screening, diagnosis, treatment or health interventions
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
| [20] | Chiappini, E., Bortone, B., Galli, L. & de Martino, M. Guidelines for the Symptomatic Management of Fever in Children: Systematic Review of the Literature and Quality Appraisal with AGREE II. BMJ Open. 2017, 7(7), e015404.
https://doi.org/10.1136/bmjopen-2016-015404 |
| [21] | Könsgen, N., Barcot, O., Heß, S., Puljak, L., Goossen, K., Rombey, T., et al. Inter-Review Agreement of Risk-of-Bias Judgments Varied in Cochrane Reviews. J Clin Epidemiol. 2020, 120, 25–32.
https://doi.org/10.1016/j.jclinepi.2020.01.004 |
[16, 20, 21]
. Furthermore, it can be used to develop, report and evaluate evidence-based guidelines
| [12] | Zeng, X., Zhang, Y., Kwong, J. S., Zhang, C., Li, S., Sun, F., et al. The Methodological Quality Assessment Tools for Preclinical and Clinical Studies, Systematic Review and Meta-Analysis, and Clinical Practice Guideline: A Systematic Review. J Evid Based Med. 2015, 8(1), 2–10.
https://doi.org/10.1111/jebm.12141 |
[12]
.
The assessment using this instrument contains 23 items, involving six domains: 1. scope and objective; 2. stakeholder involvement; 3. rigor of development; 4. clarity of presentation; 5. applicability; 6. editorial Independence
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
| [20] | Chiappini, E., Bortone, B., Galli, L. & de Martino, M. Guidelines for the Symptomatic Management of Fever in Children: Systematic Review of the Literature and Quality Appraisal with AGREE II. BMJ Open. 2017, 7(7), e015404.
https://doi.org/10.1136/bmjopen-2016-015404 |
[16, 20]
. The items distributed within each domain are evaluated on a 7-point scale, ranging from completely disagree (grade 1, which is the minimum) to completely agree (grade 7, which is the maximum)
| [11] | Hoffmann-Eßer, W., Siering, U., Neugebauer, E. A., Brockhaus, A. C., Lampert, U. & Eikermann, M. Guideline Appraisal with AGREE II: Systematic Review of the Current Evidence on How Users Handle the 2 Overall Assessments. PLoS ONE. 2017, 12(3), e0174831.
https://doi.org/10.1371/journal.pone.0174831 |
[11]
.
The scores for the evaluated domains are calculated by summing all the scores for the individual items, including the scores given by all the evaluators, then scaling the total as a percentage of the maximum possible score for the domain
| [11] | Hoffmann-Eßer, W., Siering, U., Neugebauer, E. A., Brockhaus, A. C., Lampert, U. & Eikermann, M. Guideline Appraisal with AGREE II: Systematic Review of the Current Evidence on How Users Handle the 2 Overall Assessments. PLoS ONE. 2017, 12(3), e0174831.
https://doi.org/10.1371/journal.pone.0174831 |
[11]
. The calculation of the percentage achieved in the domains follows the formula: ((Score obtained – Minimum score) / (Maximum score – Minimum score)) x 100. For a better visualization of a general overview of the evaluated domains, an arithmetic average is calculated with the percentages achieved by all guidelines, going domain by domain
| [11] | Hoffmann-Eßer, W., Siering, U., Neugebauer, E. A., Brockhaus, A. C., Lampert, U. & Eikermann, M. Guideline Appraisal with AGREE II: Systematic Review of the Current Evidence on How Users Handle the 2 Overall Assessments. PLoS ONE. 2017, 12(3), e0174831.
https://doi.org/10.1371/journal.pone.0174831 |
[11]
.
It is important to highlight that this instrument does not provide a specific parameter for recommending or not recommending protocols. However, the item Rigor of development is addressed as the main evaluation parameter in the literature consulted and the higher this item scores, the better the quality of the guideline
| [11] | Hoffmann-Eßer, W., Siering, U., Neugebauer, E. A., Brockhaus, A. C., Lampert, U. & Eikermann, M. Guideline Appraisal with AGREE II: Systematic Review of the Current Evidence on How Users Handle the 2 Overall Assessments. PLoS ONE. 2017, 12(3), e0174831.
https://doi.org/10.1371/journal.pone.0174831 |
| [15] | AGREE Next Steps Consortium. The AGREE II Instrument. 2009. Available from: http://www.agreetrust.org (Accessed 2020 Aug 24). |
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
| [21] | Könsgen, N., Barcot, O., Heß, S., Puljak, L., Goossen, K., Rombey, T., et al. Inter-Review Agreement of Risk-of-Bias Judgments Varied in Cochrane Reviews. J Clin Epidemiol. 2020, 120, 25–32.
https://doi.org/10.1016/j.jclinepi.2020.01.004 |
[11, 15, 16, 21]
. Furthermore, based on criteria suggested by other authors and interpreted as relevant, a minimum score of 50% for this item is accepted in this assessment
| [8] | Migowski, A. Methodological Guidelines: Preparation of Clinical Guidelines. Rev Bras Cancerol. 2016, 62, 165–166. |
| [11] | Hoffmann-Eßer, W., Siering, U., Neugebauer, E. A., Brockhaus, A. C., Lampert, U. & Eikermann, M. Guideline Appraisal with AGREE II: Systematic Review of the Current Evidence on How Users Handle the 2 Overall Assessments. PLoS ONE. 2017, 12(3), e0174831.
https://doi.org/10.1371/journal.pone.0174831 |
| [14] | Santana, R. S., de Oliveira Lupatini, E., Zanghelini, F., de March Ronsoni, R., Rech, N. & Leite, S. N. The Different Clinical Guideline Standards in Brazil: High Cost Treatment Diseases versus Poverty-Related Diseases. PLoS One. 2028, 13(10), e0204723.
https://doi.org/10.1371/journal.pone.0204723 |
| [15] | AGREE Next Steps Consortium. The AGREE II Instrument. 2009. Available from: http://www.agreetrust.org (Accessed 2020 Aug 24). |
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
| [21] | Könsgen, N., Barcot, O., Heß, S., Puljak, L., Goossen, K., Rombey, T., et al. Inter-Review Agreement of Risk-of-Bias Judgments Varied in Cochrane Reviews. J Clin Epidemiol. 2020, 120, 25–32.
https://doi.org/10.1016/j.jclinepi.2020.01.004 |
[8, 11, 14-16, 21]
. A guideline that scores between 30% and 50% in Rigor of Development and achieves averages above 50% in two other domains may be considered “Recommended with Modifications”. If the guideline scores less than 30% it may be considered as “Not Recommended”
| [15] | AGREE Next Steps Consortium. The AGREE II Instrument. 2009. Available from: http://www.agreetrust.org (Accessed 2020 Aug 24). |
[15]
.
2.3. Data Processing
The aspects covered by the AGREE II instrument were evaluated by four people, previously trained and familiar with this evaluation method. They classified the guidelines and/or clinical protocols using scores from 1 to 7. The results were calculated in percentage format according to the guidelines found and with the aim of evaluating the guideline recommendation in its most relevant aspects
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
[16]
.
Due to the possibility of average variation by AGREE II, generally from 0% to 100%, and considering the values found, in addition to possible human factors inherent to the evaluation, the quadratic weighted
Kappa statistic was calculated to measure the degree agreement between evaluators and increase the reliability of the process
| [15] | AGREE Next Steps Consortium. The AGREE II Instrument. 2009. Available from: http://www.agreetrust.org (Accessed 2020 Aug 24). |
| [18] | Alnamankany, A. & Ashley, P. Assessment of the Quality of Reporting of Randomized Clinical Trials in Paediatric Dentistry: A Comparative Systematic Review. Taibah Univ Med Sci. 2020, 15(1), 1–7.
https://doi.org/10.1016/j.jtumed.2019.12.001 |
| [19] | Anwer, M. A., Al-Fahed, O. B., Arif, S. I., Amer, Y. S., Titi, M. A. & Al-Rukban, M. O. Quality Assessment of Recent Evidence-Based Clinical Practice Guidelines for Management of Type 2 Diabetes Mellitus in Adults Using the AGREE II Instrument. J Eval Clin Pract. 2018, 24(1), 166–172.
https://doi.org/10.1111/jep.12832 |
[15, 18, 19]
.
To perform the calculation, grades 1 and 2 were equivalent to grade 1 for the
Kappa calculation, grades 3, 4 and 5 referred to grade 2 and grades 6 and 7 to grade 3 for calculating the
Kappa statistic, respectively
| [18] | Alnamankany, A. & Ashley, P. Assessment of the Quality of Reporting of Randomized Clinical Trials in Paediatric Dentistry: A Comparative Systematic Review. Taibah Univ Med Sci. 2020, 15(1), 1–7.
https://doi.org/10.1016/j.jtumed.2019.12.001 |
[18]
. Scores 1 and 2 were considered "low", scores between 3 and 5 "intermediate" and scores 6 and 7 "high"
| [15] | AGREE Next Steps Consortium. The AGREE II Instrument. 2009. Available from: http://www.agreetrust.org (Accessed 2020 Aug 24). |
[15]
. In addition, the following comparison parameters
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
| [22] | Bielory, L., Meltzer, E. O., Nichols, K. K., Melton, R., Thomas, R. K. & Bartlett, J. D. An Algorithm for the Management of Allergic Conjunctivitis. Allergy Asthma Proc. 2013, 34(5), 408–420. https://doi.org/10.2500/aap.2013.34.3680 |
[16, 22]
. were considered: Poor agreement (<0 .00); Mild (0.00-0.20); Fair (0.21-0.40); Moderate (0.41-0.60); Substantial (0.61-0.80) and Almost Perfect (0.81-1).
3. Results
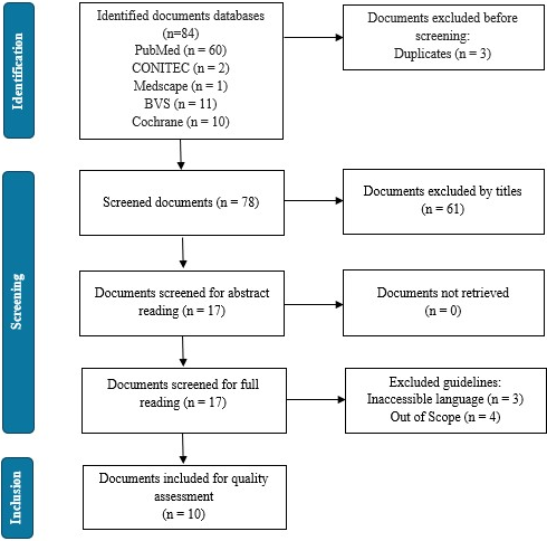
The selection of texts was checked by a reviewer, in accordance with the principle of peer review, and discrepancies were resolved by discussion between those involved. Initially, 84 texts were selected from the sources consulted, followed by evaluation of the title and abstract, as described in
Figure 1. After applying the exclusion criteria, 10 guidelines were selected for critical quality assessment.
The selected guidelines are described in
Table 1 and originate from Spain (CPG 2), Japan (CPG 4), Italy (CPG 6) and the United States of America (CPGs 7, 8 and 9). Most of the documents located refer only to the management of allergic conjunctivitis. CPG 1, 3 and 5 simultaneously address the three types of conjunctivitis included in the scope of this article. CPG 10 addresses the treatment of rhinoconjunctivitis, which is allergic conjunctivitis associated with allergic rhinitis.
Table 1.
Clinical practice guidelines for the management of conjunctivitis selected for evaluation. Clinical practice guidelines for the management of conjunctivitis selected for evaluation. Clinical practice guidelines for the management of conjunctivitis selected for evaluation. Clinical Guideline (year) | Country of origin | Group/Responsible Organization |
CPG 1 (2019) | Acute conjunctivitis | Brazil | BMJ Best Practice |
CPG 2 (2015) | Consensus document on allergic conjunctivitis (DECA) | Spain | (SEAIC 2010 Rhinoconjunctivitis Committee) and (Spanish Group Ocular Surface-GESOC) |
CPG 3 (2019) | Conjunctivitis Preferred Practice Pattern® | USA | American Academy Of Ophthalmology |
CPG 4 (2011) | Japanese guideline for allergic conjunctival diseases | Japan | Japanese Ocular Allergology Society |
CPG 5 (2013) | Conjunctivitis: a systematic review of diagnosis and treatment | USA | Department of Ophthalmology and Visual Sciences, University of Wisconsin, Madison. |
CPG 6 (2018) | Allergic conjunctivitis: current concepts on pathogenesis and management | Italy | Department of Sense Organs, University Sapienza of Rome. |
CPG 7 (2019) | ICON: Diagnosis and management of allergic conjunctivitis | USA | American College of Allergy, Asthma & Immunology |
CPG 8 (2013) | An algorithm for the management of allergic conjunctivitis | USA | Allergy and Asthma Center Medicine, Pediatrics & Ophthalmology Rutgers University Center for Climate Prediction |
CPG 9 (2012) | Management of seasonal allergic conjunctivitis: guide to therapy | USA | Acta Ophthalmologica Scandinavica Foundation |
CPG10 (2017) | EAACI Guidelines on Allergen Immunotherapy: Allergic rhinoconjunctivitis, 2017 | United Kingdom | Centre for Food Allergy Diagnosis and Treatment Veneto Region, University of Padua |
CPG: Clinical Practice Guideline; USA: United States of America.
Figure 1. Sample definition flowchart.
3.1. General Recommendations of the Guidelines
In
Table 2, it is observed that prevention is emphasized as the first line of treatment, as well as the use of various non-pharmacological measures, which aim to minimize symptoms and discomfort caused by the disease
| [1] | Sambursky, R. Acute Conjunctivitis. BMJ Best Practice. 2019, 1–55. |
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [4] | Bielory, L., Delgado, L., Katelaris, C. H., Leonardi, A., Rosario, N., & Vichyanoud, P. ICON: Diagnosis and Management of Allergic Conjunctivitis. Ann Allergy Asthma Immunol. 2020, 124(2), 118–134.
https://doi.org/10.1016/j.anai.2019.11.014 |
| [23] | Bielory, B., Brien, T. & Bielory, L. Management of Seasonal Allergic Conjunctivitis: Guide to Therapy. Acta Ophthalmol. 2012, 90(5), 399–407. |
| [24] | Palareti, G., Legnani, C., Cosmi, B., et al. EAACI Guidelines on Allergen Immunotherapy: Allergic Rhinoconjunctivitis (Position Paper). Int J Lab Hematol. 2018, 73(4), 765–798.
https://doi.org/10.1111/ijlh.12843 |
| [25] | Takamura, E., Uchio, E., Ebihara, N., Ohno, S., Ohashi, Y., Okamoto, S., et al. Japanese Guideline for Allergic Conjunctival Diseases. Allergol Int. 2011, 60(2), 191–203.
https://doi.org/10.2332/allergolint.60.191 |
| [26] | Azari, A. & Barney, N. Conjunctivitis: A Systematic Review of Diagnosis and Treatment. JAMA. 2013, 310(16), 1721–1729.
https://doi.org/10.1001/jama.2013.280318 |
| [27] | Sacchetti, M., Abicca, I., Bruscolini, A., Cavaliere, C., Nebbioso, M. & Lambiase, A. Allergic Conjunctivitis: Current Concepts on Pathogenesis and Management. J Biol Regul Homeost Agents. 2018, 32(1 Suppl. 1), 49–60.
https://doi.org/10.23812/21-3-E |
| [28] | Sánchez-Hernández, M. C., Montero, J., Rondon, C., Benitez del Castillo, J. M., Velázquez, E., Herreras, J. M., et al. Consensus Document on Allergic Conjunctivitis (DECA). J Investig Allergol Clin Immunol. 2015, 25(2), 94–106.
https://doi.org/10.18176/resp.0006 |
| [29] | Ventocilla, M. Allergic Conjunctivitis. Medscape. 2019, 1–18. |
[1, 3, 4, 23-29]
. Furthermore, educating the family and patient about adequate and simple hygiene measures, such as washing hands and not sharing personal objects, are present in three guidelines (CPGs 1, 3 and 5). These discuss minimizing the spread of contamination. Furthermore, they reinforce the importance of reporting to the patient the highly contagious nature of infectious forms of conjunctivitis. That said, they infer the need for absence from school/work during the presentation of the disease.
Table 2. Non-pharmacological treatment recommendations.
NON-PHARMACOLOGICAL TREATMENT FOR ACUTE CONJUNCTIVITIS |
Recommendation | CPG |
1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Provide initial and preventive guidance | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Maintain simple hygiene measures | Yes | No | Yes | No | Yes | No | No | No | No | No |
Use of artificial tears | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
Stop using contact lenses | No | No | No | Yes | Yes | No | Yes | No | No | No |
Cold compresses | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | No | No |
Use of sunglasses | No | Yes | Yes | Yes | No | No | No | No | No | No |
Minimize friction in the eyes | No | No | No | No | No | No | Yes | No | No | No |
Immunotherapy | No | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes |
The use of artificial tears is recommended in 90% of the guidelines evaluated, with the United Kingdom guideline (CPG 10) being the only one that disagrees. Adequate cycles of immunotherapy, sublingually or subcutaneously, are indicated in 80% of recommendations. The use of cold compresses is present in 70% of recommendations. Discontinuation of contact lens use is recommended in 30% of guidelines, within the scope of this article and not based on other existing forms of conjunctivitis. It was estimated that 30% of guidelines recommend the use of sunglasses, mainly to prevent photosensitivity and contact with allergens present in the air. And only 10% of these, that is, 1 clinical practice guideline (CPG 7), recommend minimizing friction on the eye to avoid triggering the inflammatory cascade
| [4] | Bielory, L., Delgado, L., Katelaris, C. H., Leonardi, A., Rosario, N., & Vichyanoud, P. ICON: Diagnosis and Management of Allergic Conjunctivitis. Ann Allergy Asthma Immunol. 2020, 124(2), 118–134.
https://doi.org/10.1016/j.anai.2019.11.014 |
[4]
.
Table 3. Pharmacological treatment recommendations.
PHARMACOLOGICAL TREATMENT FOR ACUTE ALLERGIC CONJUNCTIVITIS | Examples |
Drug class | CPG |
1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
Topical and systemic antihistamines | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Azelastine hydrochloride 0.05%; Loratadine; Desloratadine |
Topical decongestants | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Naphazoline hydrochloride 0.012% or 0.1% |
Topical NSAIDs | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | No | Ketorolac Tromethamine 0.5% |
Mast cell stabilizers | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Cromoglicate Sodium 2% and 4%; Lodoxamide; Tromethamine |
Corticosteroids | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Prednisone; Loteprednol etabonate 0.2% or 0.5% |
Antihistamine associated with topical decongestants | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | No | Naphazoline Hydrochloride 0.025% + Pheniramine Maleate 0.3% |
Immunosuppressant | Yes | No | Yes | Yes | No | Yes | Yes | Yes | No | No | Prednisone; Cyclosporine; Tacrolimus |
Antiretrovirals | Yes | No | Yes | No | Yes | No | No | No | No | No | Ganciclovir 0.15% |
Antibiotics | Yes | No | Yes | No | Yes | Yes | No | No | No | No | Erythromycin; Azithromycin; Polymyxin + Trimethoprim |
NSAIDs: Non-steroidal anti-inflammatory drugs; CPG: Clinical Practice Guideline.
In general, treatment refers to the use of therapy, together with the identification of the allergen and the prevention of the patient's contact with it
| [1] | Sambursky, R. Acute Conjunctivitis. BMJ Best Practice. 2019, 1–55. |
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
[1, 3]
. Identification of the causative agent of conjunctivitis allows pharmacological treatment to be more effective, directing management to its root cause
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [4] | Bielory, L., Delgado, L., Katelaris, C. H., Leonardi, A., Rosario, N., & Vichyanoud, P. ICON: Diagnosis and Management of Allergic Conjunctivitis. Ann Allergy Asthma Immunol. 2020, 124(2), 118–134.
https://doi.org/10.1016/j.anai.2019.11.014 |
[3, 4]
. The most prevalent pharmacological recommendations in the management of this disorder are described in
Table 3. Topical antihistamines, systemic antihistamines, corticosteroids and topical decongestants are recommended in 100% of the clinical practice protocols evaluated. Preference is given to the topical presentation of these medications, but there are systemic alternatives presented
| [4] | Bielory, L., Delgado, L., Katelaris, C. H., Leonardi, A., Rosario, N., & Vichyanoud, P. ICON: Diagnosis and Management of Allergic Conjunctivitis. Ann Allergy Asthma Immunol. 2020, 124(2), 118–134.
https://doi.org/10.1016/j.anai.2019.11.014 |
[4]
.
The use of mast cell stabilizers is recommended in 90% of the guidelines, non-steroidal anti-inflammatory drugs (NSAIDs) in 80%. Dual-action agents, which combine topical antihistamines and topical decongestants, are recommended in 80% of CPGs, immunosuppressants in 60%, antibiotics in 40% and antiretrovirals in 30% of clinical practice guidelines evaluated.
Regarding topical antihistamines, azelastine hydrochloride 0.05% is recommended
| [5] | DynaMed. Record No. Infectious Conjunctivitis. Ipswich, MA: EBSCO Information Services; 1995, updated 2018. Available from:
https://www.dynamed.com/topics/dmpANT116741 (Accessed 2020 Jan 06). |
| [27] | Sacchetti, M., Abicca, I., Bruscolini, A., Cavaliere, C., Nebbioso, M. & Lambiase, A. Allergic Conjunctivitis: Current Concepts on Pathogenesis and Management. J Biol Regul Homeost Agents. 2018, 32(1 Suppl. 1), 49–60.
https://doi.org/10.23812/21-3-E |
[5, 27]
. The corticosteroids prednisone and lojaprednol etabonate 0.2% or 0.5%
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [5] | DynaMed. Record No. Infectious Conjunctivitis. Ipswich, MA: EBSCO Information Services; 1995, updated 2018. Available from:
https://www.dynamed.com/topics/dmpANT116741 (Accessed 2020 Jan 06). |
| [24] | Palareti, G., Legnani, C., Cosmi, B., et al. EAACI Guidelines on Allergen Immunotherapy: Allergic Rhinoconjunctivitis (Position Paper). Int J Lab Hematol. 2018, 73(4), 765–798.
https://doi.org/10.1111/ijlh.12843 |
| [29] | Ventocilla, M. Allergic Conjunctivitis. Medscape. 2019, 1–18. |
[3, 5, 24, 29]
. Of the topical decongestants, deafazoline hydrochloride 0.012% or 0.1% was recommended
| [24] | Palareti, G., Legnani, C., Cosmi, B., et al. EAACI Guidelines on Allergen Immunotherapy: Allergic Rhinoconjunctivitis (Position Paper). Int J Lab Hematol. 2018, 73(4), 765–798.
https://doi.org/10.1111/ijlh.12843 |
| [29] | Ventocilla, M. Allergic Conjunctivitis. Medscape. 2019, 1–18. |
[24, 29]
. As for systemic antihistamines, there is still a predilection for second-generation presentations, such as loratadine, desloratadine and fexofenadine hydrochloride, which have fewer associated adverse effects
| [1] | Sambursky, R. Acute Conjunctivitis. BMJ Best Practice. 2019, 1–55. |
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [24] | Palareti, G., Legnani, C., Cosmi, B., et al. EAACI Guidelines on Allergen Immunotherapy: Allergic Rhinoconjunctivitis (Position Paper). Int J Lab Hematol. 2018, 73(4), 765–798.
https://doi.org/10.1111/ijlh.12843 |
| [29] | Ventocilla, M. Allergic Conjunctivitis. Medscape. 2019, 1–18. |
| [30] | Hamrah, P. & Dana, R. Allergic Conjunctivitis: Management. Am J Ophthalmol. 1951, 34, 1046. |
| [31] | Hamrah, A. P. & Dana, R. Vernal Keratoconjunctivitis. UpToDate. 2020, 1–21. |
[1, 3, 24, 29-31]
.
Furthermore, among mast cell stabilizers, 2% and 4% sodium cromoglycate and lodoxamide tromethamine
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [5] | DynaMed. Record No. Infectious Conjunctivitis. Ipswich, MA: EBSCO Information Services; 1995, updated 2018. Available from:
https://www.dynamed.com/topics/dmpANT116741 (Accessed 2020 Jan 06). |
| [23] | Bielory, B., Brien, T. & Bielory, L. Management of Seasonal Allergic Conjunctivitis: Guide to Therapy. Acta Ophthalmol. 2012, 90(5), 399–407. |
| [24] | Palareti, G., Legnani, C., Cosmi, B., et al. EAACI Guidelines on Allergen Immunotherapy: Allergic Rhinoconjunctivitis (Position Paper). Int J Lab Hematol. 2018, 73(4), 765–798.
https://doi.org/10.1111/ijlh.12843 |
| [26] | Azari, A. & Barney, N. Conjunctivitis: A Systematic Review of Diagnosis and Treatment. JAMA. 2013, 310(16), 1721–1729.
https://doi.org/10.1001/jama.2013.280318 |
| [27] | Sacchetti, M., Abicca, I., Bruscolini, A., Cavaliere, C., Nebbioso, M. & Lambiase, A. Allergic Conjunctivitis: Current Concepts on Pathogenesis and Management. J Biol Regul Homeost Agents. 2018, 32(1 Suppl. 1), 49–60.
https://doi.org/10.23812/21-3-E |
| [29] | Ventocilla, M. Allergic Conjunctivitis. Medscape. 2019, 1–18. |
[3, 5, 23, 24, 26, 27, 29]
are recommended. Of the non-steroidal anti-inflammatory drugs (NSAIDs), ketorolac tromethamine 0.5% is recommended
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [24] | Palareti, G., Legnani, C., Cosmi, B., et al. EAACI Guidelines on Allergen Immunotherapy: Allergic Rhinoconjunctivitis (Position Paper). Int J Lab Hematol. 2018, 73(4), 765–798.
https://doi.org/10.1111/ijlh.12843 |
| [27] | Sacchetti, M., Abicca, I., Bruscolini, A., Cavaliere, C., Nebbioso, M. & Lambiase, A. Allergic Conjunctivitis: Current Concepts on Pathogenesis and Management. J Biol Regul Homeost Agents. 2018, 32(1 Suppl. 1), 49–60.
https://doi.org/10.23812/21-3-E |
| [29] | Ventocilla, M. Allergic Conjunctivitis. Medscape. 2019, 1–18. |
[3, 24, 27, 29]
. Of the dual-action agents, the most recommended is naphazoline hydrochloride 0.025% associated with pheniramine maleate 0.3%
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [5] | DynaMed. Record No. Infectious Conjunctivitis. Ipswich, MA: EBSCO Information Services; 1995, updated 2018. Available from:
https://www.dynamed.com/topics/dmpANT116741 (Accessed 2020 Jan 06). |
| [24] | Palareti, G., Legnani, C., Cosmi, B., et al. EAACI Guidelines on Allergen Immunotherapy: Allergic Rhinoconjunctivitis (Position Paper). Int J Lab Hematol. 2018, 73(4), 765–798.
https://doi.org/10.1111/ijlh.12843 |
[3, 5, 24]
. Within the group of immunosuppressants, prednisone, cyclosporine or tacrolimus are mentioned
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
[3]
. Of the antibiotics, erythromycin, azithromycin or polymyxin/trimethoprim drops
| [3] | Varu, D. M., Rhee, M. K., Akpek, E. K., Amescua, G., Farid, M., Garcia-Ferrer, F. J., et al. Conjunctivitis Preferred Practice Pattern®. Ophthalmology. 2019, 126(1), P94–P169.
https://doi.org/10.1016/j.ophtha.2018.10.023 |
| [5] | DynaMed. Record No. Infectious Conjunctivitis. Ipswich, MA: EBSCO Information Services; 1995, updated 2018. Available from:
https://www.dynamed.com/topics/dmpANT116741 (Accessed 2020 Jan 06). |
[3, 5]
. And, finally, the antiretroviral drug ganciclovir 0.15%
| [1] | Sambursky, R. Acute Conjunctivitis. BMJ Best Practice. 2019, 1–55. |
[1]
.
3.2. Assessment of the Quality of Guidelines Using the AGREE II Instrument
After evaluating the criteria by AGREE II, the average reported for each of the six domains of each protocol/clinical guideline was calculated. The averages can be seen in
Table 4. After applying the selected criteria, it was found that clinical practice guidelines 2, 3, 5, and 10 were considered recommended to be used in the practice of health professionals and demonstrated superior development quality the rest. Clinical practice guidelines 1, 4, 6, 7, 8 and 9 must undergo evaluation and review of the methodological criteria for elaboration for subsequent recommendation.
Table 4. Scores for each domain of the AGREE II instrument.
Guideline | Scope and Purpose | Stakeholder involvement | Rigor of Development | Clarity of presentation | Applicability | Editorial independence | Recommendation |
CPG 1 | 11% | 38% | 30% | 94% | 17% | 13% | Not Recommended |
CPG 2 | 85% | 60% | 67% | 92% | 14% | 88% | Recommended |
CPG 3 | 94% | 72% | 80% | 93% | 31% | 100% | Recommended |
CPG 4 | 15% | 25% | 11% | 60% | 0% | 0% | Not Recommended |
CPG 5 | 65% | 35% | 64% | 92% | 9% | 100% | Recommended |
CPG 6 | 19% | 22% | 9% | 51% | 5% | 71% | Not Recommended |
CPG 7 | 56% | 40% | 21% | 85% | 11% | 100% | Not Recommended |
CPG 8 | 44% | 26% | 17% | 75% | 7% | 50% | Not Recommended |
CPG 9 | 18% | 19% | 18% | 65% | 1% | 13% | Not Recommended |
CPG 10 | 96% | 99% | 91% | 96% | 93% | 100% | Recommended |
AVERAGE | 50% | 44% | 41% | 80% | 19% | 64% | - |
The first domain evaluated, Scope and Purpose, addresses the general objective of the guideline and the target population, obtaining an overall average of 50.3%. Guidelines 2, 3, 5, 7 and 10 presented an average of more than 50%, covering the general objectives of identification, classification, treatment and prevention in a clear and specific way. On the other hand, CPGs 1, 4, 6 and 9 presented an average evaluation of less than 20%, with a description of the general objective that was little recognized by the evaluators without a description of the recipient of such a guideline.
In the second domain, Stakeholder Involvement, only CPGs 2, 3 and 10 achieved averages above 50%, with target users referred to as doctors and/or healthcare specialists. This item had an overall average of 43.6. For the other texts, there was a variability in averages from 19% to 40%, where the sub-item Knowledge About the Opinions and Preferences of the Target Population can be highlighted as one of the reasons for the low grades. These averages can also infer a development team that does not cover all relevant groups of professionals, being restricted to specialist doctors. Furthermore, the description of target users can be described more clearly in future revisions.
The Rigor of Development in the references consulted is addressed as the main assessment item in a guideline
| [8] | Migowski, A. Methodological Guidelines: Preparation of Clinical Guidelines. Rev Bras Cancerol. 2016, 62, 165–166. |
| [11] | Hoffmann-Eßer, W., Siering, U., Neugebauer, E. A., Brockhaus, A. C., Lampert, U. & Eikermann, M. Guideline Appraisal with AGREE II: Systematic Review of the Current Evidence on How Users Handle the 2 Overall Assessments. PLoS ONE. 2017, 12(3), e0174831.
https://doi.org/10.1371/journal.pone.0174831 |
| [14] | Santana, R. S., de Oliveira Lupatini, E., Zanghelini, F., de March Ronsoni, R., Rech, N. & Leite, S. N. The Different Clinical Guideline Standards in Brazil: High Cost Treatment Diseases versus Poverty-Related Diseases. PLoS One. 2028, 13(10), e0204723.
https://doi.org/10.1371/journal.pone.0204723 |
| [15] | AGREE Next Steps Consortium. The AGREE II Instrument. 2009. Available from: http://www.agreetrust.org (Accessed 2020 Aug 24). |
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
| [21] | Könsgen, N., Barcot, O., Heß, S., Puljak, L., Goossen, K., Rombey, T., et al. Inter-Review Agreement of Risk-of-Bias Judgments Varied in Cochrane Reviews. J Clin Epidemiol. 2020, 120, 25–32.
https://doi.org/10.1016/j.jclinepi.2020.01.004 |
[8, 11, 14-16, 21]
. This parameter must be considered carefully and transparently
| [8] | Migowski, A. Methodological Guidelines: Preparation of Clinical Guidelines. Rev Bras Cancerol. 2016, 62, 165–166. |
| [15] | AGREE Next Steps Consortium. The AGREE II Instrument. 2009. Available from: http://www.agreetrust.org (Accessed 2020 Aug 24). |
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
[8, 15, 16]
.
The overall average for this item was 40.8%, the second lowest overall average within the criteria evaluated. This corresponds to an insufficient description of the methodological rigor applied and/or a lack of description regarding the selection of evidence on which its recommendations were based. In this regard, 5 guidelines presented an average of less than 30% in this domain.
The only item that obtained an overall average lower than the Rigor of Development was the one corresponding to “Applicability”, an item capable of evaluating the application and monitoring tools of the recommendations contained in the guideline. With an average of 18.8%, the scores can be attributed to the lack of information such as: possible barriers to applying the guideline, estimated costs and conditions for monitoring it. Application costs, as well as tools for this and monitoring, were only described in CPG 10.
Furthermore, the AGREE II assessment items “Clarity of Presentation” and “Editorial Independence” reached the highest averages of the assessments carried out, representing, respectively, 80.3% and 70.6%, which corroborates the recommendation of the CPGs 2, 3, 5, and 10, which also presented averages above 50% in the item “Development Rigor”.
4. Discussion
Among the guidelines evaluated, 40% were considered “recommended” and, within the criteria established in this article, none demonstrated the need for immediate improvements in their application. This infers that 4 of the 10 guidelines evaluated by the AGREE II method achieved satisfactory scores in the main items established for the preparation of clinical practice guideline
| [17] | Vaz, J. M., Alves, B. M., Duarte, D. B., Marques, L. A. & Santana, R. S. Quality Appraisal of Existing Guidelines for the Management of Headache Disorders by the AGREE II’s Method. Cephalalgia. 2022, 42(3), 239–249.
https://doi.org/10.1177/03331024211056694 |
| [18] | Alnamankany, A. & Ashley, P. Assessment of the Quality of Reporting of Randomized Clinical Trials in Paediatric Dentistry: A Comparative Systematic Review. Taibah Univ Med Sci. 2020, 15(1), 1–7.
https://doi.org/10.1016/j.jtumed.2019.12.001 |
[17, 18]
.
Among the non-pharmacological and pharmacological recommendations, there is uniformity in the recommendations addressed. Since the guidelines evaluated originate from different countries, this demonstrates greater reliability of application in clinical practice. All non-pharmacological recommendations present benefits capable of outweighing any risks they may cause, although not all of them present a high level of evidence. Furthermore, non-pharmacological therapies are efficient in controlling symptoms related to acute conjunctivitis and are the first-line treatment of the disease
| [17] | Vaz, J. M., Alves, B. M., Duarte, D. B., Marques, L. A. & Santana, R. S. Quality Appraisal of Existing Guidelines for the Management of Headache Disorders by the AGREE II’s Method. Cephalalgia. 2022, 42(3), 239–249.
https://doi.org/10.1177/03331024211056694 |
| [18] | Alnamankany, A. & Ashley, P. Assessment of the Quality of Reporting of Randomized Clinical Trials in Paediatric Dentistry: A Comparative Systematic Review. Taibah Univ Med Sci. 2020, 15(1), 1–7.
https://doi.org/10.1016/j.jtumed.2019.12.001 |
[17, 18]
.
The pharmacological recommendations in the guidelines are well designed and aligned. These are mainly aimed at symptomatic relief of the disease, although some medications reduce the duration of its course, such as the recommendation of the use of antibiotics to manage bacterial infectious conjunctivitis, an indication contained in CPGs 1, 3, 5 and 6, and which presents a high level of evidence, but with a weak recommendation. Furthermore, it is worth noting that the use of antibiotics is not indicated for allergic and viral forms of conjunctivitis
| [17] | Vaz, J. M., Alves, B. M., Duarte, D. B., Marques, L. A. & Santana, R. S. Quality Appraisal of Existing Guidelines for the Management of Headache Disorders by the AGREE II’s Method. Cephalalgia. 2022, 42(3), 239–249.
https://doi.org/10.1177/03331024211056694 |
| [18] | Alnamankany, A. & Ashley, P. Assessment of the Quality of Reporting of Randomized Clinical Trials in Paediatric Dentistry: A Comparative Systematic Review. Taibah Univ Med Sci. 2020, 15(1), 1–7.
https://doi.org/10.1016/j.jtumed.2019.12.001 |
| [21] | Könsgen, N., Barcot, O., Heß, S., Puljak, L., Goossen, K., Rombey, T., et al. Inter-Review Agreement of Risk-of-Bias Judgments Varied in Cochrane Reviews. J Clin Epidemiol. 2020, 120, 25–32.
https://doi.org/10.1016/j.jclinepi.2020.01.004 |
[17, 18, 21]
.
Furthermore, there is no specific therapy for the treatment of viral infectious conjunctivitis and systemic agents do not play any therapeutic role in their management. The recommended topical antiretroviral, ganciclovir 0.15%, is used in specific cases due to adenovirus contamination. That said, we can infer one of the reasons why there are more clinical management guidelines focused on allergic conjunctivitis compared to others.
In severe cases, clinical management incorporates a drug combination. Thus, corticosteroids can be recommended, with loteprednol etabonate having fewer adverse effects compared to other examples, such as prednisolone. The use of this pharmacological class carries several associated risks and should only be carried out under medical supervision. Furthermore, it is emphasized in the evaluated guidelines that the chronic use of any non-pharmacological and pharmacological option presented is not recommended.
In general, support measures are low value and can be financially accessible for most of the population, except for immunotherapy, which is a treatment with a higher cost than others. Furthermore, minimizing friction on the eye to avoid triggering the inflammatory cascade can be considered a valid recommendation, which application would not cause harm to patients and, if aimed at infectious forms, could prevent the spread of pathogens to surfaces and even reduce or delay the involvement of the second eye.
It was observed that the United States of America has 50% of published protocols for the clinical management of conjunctivitis, which can be justified by the high prevalence of the disease in its population and, also, by the consolidation of evidence-based healthcare in this country, with the high prevalence of development and implementation of clinical protocols and therapeutic guidelines guiding health care. The other 5 guidelines come from different countries and do not present statistical data estimating the epidemiological impact on their country of origin.
The United Kingdom guideline, alone, presented the best averages in all evaluated criteria, reaching a value above 90%. This guideline addresses the treatment of rhinoconjunctivitis. Its production followed the elaboration model of the AGREE II instrument, which justifies its higher averages compared to other CPGs. Furthermore, its applicability with regard specifically to the management of acute allergic, bacterial and viral conjunctivitis can be considered limited, if used in isolation, that is, it presents limited non-pharmacological and pharmacological options compared to other guidelines.
CPGs 2, 4, 6, 7, 9 and 10 refer only to the management of allergic conjunctivitis and when they address other types of conjunctivitis, they provide a theoretical definition and not the management specifically. CPGs 1, 3 and 5 address the three types of conjunctivitis included in the scope of this article. It is also noted that none of the guidelines selected and evaluated address the importance of pharmaceutical care, demonstrating fragility regarding the management of conjunctivitis as a self-limited health problem that can be treated within the scope of community pharmacies.
However, there is a lack of protocols with clear objectives and high-quality development regarding the three main types of acute conjunctivitis analyzed, causing difficulty in implementing the recommendations mentioned in clinical guidelines. This is demonstrated in what corresponds to the evaluated item “Applicability”, which obtained the lowest general average, which corresponded to 18.8% of the evaluation, even with a variation from 0 to 93%. The main reasons for such a low average are the lack of items identified as facilitators and/or barriers inherent to the application of the adopted recommendations, the costs involved or the lack of establishing criteria for monitoring them after the recommendations
| [17] | Vaz, J. M., Alves, B. M., Duarte, D. B., Marques, L. A. & Santana, R. S. Quality Appraisal of Existing Guidelines for the Management of Headache Disorders by the AGREE II’s Method. Cephalalgia. 2022, 42(3), 239–249.
https://doi.org/10.1177/03331024211056694 |
| [18] | Alnamankany, A. & Ashley, P. Assessment of the Quality of Reporting of Randomized Clinical Trials in Paediatric Dentistry: A Comparative Systematic Review. Taibah Univ Med Sci. 2020, 15(1), 1–7.
https://doi.org/10.1016/j.jtumed.2019.12.001 |
| [21] | Könsgen, N., Barcot, O., Heß, S., Puljak, L., Goossen, K., Rombey, T., et al. Inter-Review Agreement of Risk-of-Bias Judgments Varied in Cochrane Reviews. J Clin Epidemiol. 2020, 120, 25–32.
https://doi.org/10.1016/j.jclinepi.2020.01.004 |
[17, 18, 21]
.
Furthermore, 50% of clinical practice guidelines presented a Rigor of Development of less than 30%, which falls outside the criteria adopted for their recommendation. Regarding this domain, the main cause for low averages is related to insufficient description of the methods used in the construction of protocols and their listed recommendations
| [17] | Vaz, J. M., Alves, B. M., Duarte, D. B., Marques, L. A. & Santana, R. S. Quality Appraisal of Existing Guidelines for the Management of Headache Disorders by the AGREE II’s Method. Cephalalgia. 2022, 42(3), 239–249.
https://doi.org/10.1177/03331024211056694 |
| [18] | Alnamankany, A. & Ashley, P. Assessment of the Quality of Reporting of Randomized Clinical Trials in Paediatric Dentistry: A Comparative Systematic Review. Taibah Univ Med Sci. 2020, 15(1), 1–7.
https://doi.org/10.1016/j.jtumed.2019.12.001 |
| [21] | Könsgen, N., Barcot, O., Heß, S., Puljak, L., Goossen, K., Rombey, T., et al. Inter-Review Agreement of Risk-of-Bias Judgments Varied in Cochrane Reviews. J Clin Epidemiol. 2020, 120, 25–32.
https://doi.org/10.1016/j.jclinepi.2020.01.004 |
[17, 18, 21]
. The Brazilian guideline presents an average Rigor of Development assessment of 30%. However, it does not cover the other criteria to be included in the “Recommended with modifications” criteria, as, in addition to this, only the Clarity in Presentation item is greater than 50% and, therefore, the document is assigned the “Not Recommended” category”.
The quadratic weighted
Kappa coefficient found was 0.51, which fits into a moderate agreement between the evaluators and, also, a well-accepted average for evaluation according to the references consulted
| [16] | Field, M. & Lohr, K. Clinical Practice Guidelines: Directions for a New Program. Institute of Medicine. 1990. |
[16]
. Furthermore, there were no significant disagreements between the evaluators during the evaluation via AGREE II, which reinforces the
Kappa agreement found.
The quality of health care in the management of acute conjunctivitis is linked to the quality and updating of clinical guidelines. Symptomatic control of the disease can be achieved through the application of simple and/or low-cost measures. To achieve this, the guideline must cover all available therapeutic options. Updates regarding non-pharmacological therapy should be considered and prioritized in routine reviews, regarding the risk/benefit of its application, as these can control and minimize the uncomfortable symptoms of the disorder. Furthermore, expanding options for pharmacological management should be considered.
The quality of the guidelines evaluated, within the established criteria, was below expectations, although 4 guidelines achieved satisfactory grades for recommendation. In addition to the “Rigor of Development” domain, other evaluated domains had low scores, including “Applicability” and the subitem “Monitoring of Interventions”. This data should be considered when proposing future clinical guidelines to provide better healthcare for patients. The guidelines from the United States of America, for the most part, demonstrated levels below expectations, as did the guideline from Japan and Italy. The United Kingdom guideline, alone, presented the best averages in all evaluated criteria.